You’ve heard it before: medical cannabis can’t be approved because there is not enough research. Well, recently I sat through about 40 hours of conference presentations consisting of mainly cannabis researchers and heard some wonderful presentations about current research into cannabis. There is no doubt that we know a lot about cannabis and that it can dramatically alter the course of some human afflictions ranging from acne to glioblastomas. And we all want to understand the precise mechanisms at work, don’t we? I mean, it is really important to know just what exactly is happening with cannabis because all approved medical drugs are totally understood before they are released to the public, right?
Well, if you believe that final sentence I would refer you to this Wikipedia page entitled “Drugs with unknown mechanisms of action” and I think you will be surprised at the number of commonly used medications on that page.
It made me realize the self-fulfilling prophecy that has been woven into the fabric of cannabis policy. It has become obvious that there will never be enough research because: 1) the cannabis plant is a vast repository of wonderful opportunities for those who like to discover things, and 2) researchers never think there is enough research. After all, it is what they do.
Unfortunately this rather natural stance of researchers falls right into line with the best tool that governments have to maintain the tattered prohibition of cannabis — the time worn mantra “there’s not enough research.” Researchers can’t be faulted for including the phrase in nearly every presentation because it is what they do …more research. If cannabis had been proven to be a dangerous substance there would be good reason to restrict its use. A good analogy is the plant foxglove, digitalis purpurea, from which the heart medicine digitalis is derived. Telling heart patients to grow and prepare their own digitalis from the lovely foxglove plant is a true recipe for disaster. Heart patients would be dying by the score due to the toxicity of foxglove.
But cannabis isn’t foxglove. It is extraordinarily safe. The lethal dose of cannabis has cannot be calculated nor are the adverse side-effects particularly adverse (sleepiness, being the most prevalent). Doctors can safely use cannabis but, sadly, most doctors fall back on the mantra — there’s not enough research.

Not all doctors, of course. There is a growing number of physicians who have looked at the cannabis research and made the determination that there is enough research to safely recommend cannabis. Three of these doctors spoke at the recent London Congress on Clinical Trials in Cannabis, two Americans and a British oncologist. Their presentations were easily the most compelling, particularly Dr. Bonni Goldstein, a California pediatrician, who has used cannabis in the treatment of patients ranging from six weeks to 90 years in age. She and Jeff Hergenrather, another California physician, presented compelling case studies of patients who have successfully used cannabis. To these patients and their families there is plenty of research, it has been conducted in front of their very eyes and they were willing participants.
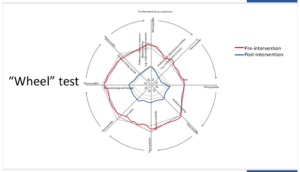
It is that latter point that Dr. Marcia Schofield of West Suffolk emphasized. She spoke of the need to re-focus our research goals to what is important to the patient and not the clinician. She made a compelling argument that studying cannabis with traditional randomly controlled trials is not the answer. “To my eyes it’s a no brainer,” she said, “we’re not using the right kind of mathematics” to collect information. She advocated for the use of Dolo Test, a pain and quality of life assessment tool developed to facilitate the understanding between clinicians and their patients. Adoption of such a tool not only helps the attending physician but the data can be shared by municipalities and hospitals to gain better insight into the effects of certain treatments.
Whether such a tool will be adopted by cannabis researchers remains to be seen but it is clear that the we-need-more-research mantra has become an impediment to the release of medical cannabis. Governments will do what they have to do to maintain their supposed control of cannabis but at what cost? As Jeff Hergenrather said, “Government control of plants, I don’t get that. … The misinformation, the deception, the ignorance and fear that are propagated in order to keep the status quo, that’s just unethical.” ❖